After Spokane group home’s closure, parents of children with intensive medical issues struggle to find support they need

Cami Flaget remembers holding her daughter, Cierra, one evening just a few weeks after bringing her home from the neonatal intensive care unit. She suddenly started turning blue, and Flaget remembers her horror as she realized her baby could be dying in her arms. Her oxygen levels had dropped, and she did not appear to be breathing.
A few long moments later, color returned to Cierra’s face. From the time her baby girl was hours old, Cami knew life with Cierra meant her child could die at any instant.

Cierra was diagnosed with a rare ring chromosome 18 disorder, and also had trouble with her heart and lungs. She needed an oxygen nasal tube to breathe and a “g-tube” connected to her stomach to keep her fed. When Cierra left the newborn intensive care unit, or NICU, after 83 days in early 2008, she had about 10 different diagnoses but would eventually end up with close to 50, Flaget estimated.
Owen Gibson’s room is in the basement level of his family’s split-level home in north Spokane. The shelves and cabinets in his room are full of catheters, filters, diapers, feeding supplies and specialty medical equipment.
He has machines, like his ventilator and humidifier for his lungs, set up in the back of his room. He has a special chair that he can sit in every day, aware and looking around, although he cannot blink and is legally blind.

Owen has a 5th chromosome deletion that limits his ability to speak or walk on his own. So far, his parents have yet to find another matching case for his specific chromosome deletion in the world.
Owen is 9 years old, and he only weighs 36 pounds. One afternoon this fall, as he wakes up from a nap, he looks around, responding to the sound of his mother’s voice. He loves listening to conversation, his mother and longtime nurse said.
Sam and Colleen Grove know both sides of care for medically fragile kids in Washington state. They had nurses in their home for the first nine years of their son Isaac’s life, then used a group care home for a few years. Isaac weighed only 2.5 pounds when he was born, and spent the first four months of his life in the NICU. His father jokes that Issac was “the old man on campus” when they finally got to bring him home.
Isaac has a rare chromosome disorder. He also has a tracheostomy – a medical breathing tube inserted in the windpipe that helps him breathe – and a feeding tube as well. His parents estimate he spent seven months of his first year in and out of the hospital, a period of pain for their son as physicians and specialists performed numerous procedures on him.

Caring for children with intensive medical needs is difficult for families, especially when the best place they are cared for is at home.
Living rooms turn into hospital rooms, and medical equipment and supplies fill spare closets. Teachers and Realtors, who are also parents, add “medical expert” to their résumés as they navigate a labyrinth of state agencies in order to get the care their children need and qualify for.
The only group care home available for families with medically intensive children in northeastern Washington closed this summer, after the Department of Children, Youth, and Families suspended its license following several injuries and incidents reported there. The closure left families with difficult decisions.
For Isaac, the closure meant either going home, to a medical foster parent, to the hospital or to another group home, hours away. While home care is the preferred option for medically intensive children, group homes are sometimes the only option, especially for families who are strained for resources or need a break or if a child requires 24-hour care.
Ultimately, Sam and Colleen Grove brought their son home, but his father is on a mission to make group care available in the region soon.
Caring for Isaac
When Isaac came home from the NICU, Colleen Grove learned the ins and outs of his care – how to suction his breathing tube to keep his airway clear, and how to bathe him safely. The family home is multi-level, and Isaac takes about 25 percent of the space, whether he is in the living room or on the upper level. Today, his space is upstairs, with his room, a bathroom and a spare bedroom that doubles as his play room.
Isaac loves Elmo and has his favorite cartoons. The Groves have installed a television above his safety bed in his room. While he cannot walk or feed himself, Isaac is expressive and generally happy. He loves when his mother sings to him, as she has his entire life.

Isaac only qualified for 10 hours of nursing per day when he first came home, which meant the Groves covered the rest, in two 7-hour shifts, as they continued learning how to feed, bathe, administer medications, schedule doctor appointments and change Isaac’s diaper – all while ensuring he continued to breathe clearly. After many appeals, with Isaac’s intensive medical needs, he qualified for 16 hours of in-home nursing care per day, the most allowable under Medicaid reimbursement guidelines.
Even with 16 hours approved, the Groves struggled to fill their schedule with at-home nurses for the first few years.
Washington requires that registered nurses provide at-home care for medically intensive children. T There is a nurse and nursing assistant shortage in Washington state, 2019 survey results from the Sentinel Network show. With hospitals competing for the same nursing graduates as home-health care agencies – and often offering higher salaries – there is a shortage of nurses willing and able to work in homes. This is true nationwide, particularly in pediatric home health care.
“The primary challenge of the pediatric home health care crisis is to develop a trained and adequately compensated workforce to meet the needs of children and their families,” a 2019 analysis published in Health Affairs said.
The Washington Legislature has worked to increase reimbursement rates for at-home nursing care, including some pay bumps that will go into effect in 2020, which parents hope will ease the stress of finding nurses and filling hours.
At-home nursing does not always pan out, however. When Isaac was 9 years old, the Groves hit a breaking point. They decided to place Isaac in a group care home.
Weeping Ridge North group care home was the only option in Spokane, and Sam and Colleen Groves made the tough decision to place Isaac there full-time.
Parents of medically fragile children are quick to admit that providing for their children puts a strain on their marriages; for single parents it can be all-consuming, and a group care home could be the only option.
Left with nothing
Isaac stayed at Weeping Ridge for nearly three years. Sam and Colleen, who could visit him at all hours, would go see him every Sunday after church and visit him throughout the week.
Group care homes for medically fragile children are licensed by the Department of Youth, Children, and Families, and while these homes must employ registered nurses, certified nursing assistants can also help provide care, a difference between group care and at-home care.
Group homes are regularly inspected, and several incidents at Weeping Ridge North led to the suspension of its license this past summer, records obtained by The Spokesman-Review show. Nine children were living at the care home when it closed, and they were all transferred to other care homes out of the area, or to hospitals to be held until a spot could be found for them, DCYF records show.
DCYF sent Israel Rodriguez, the owner of Weeping Ridge North, a letter on July 5, documenting four incidents with active investigations that happened from late April to June of this year. .
Sacred Heart Hospital staff found burn marks on one child caused by hot water in a shower; Weeping Ridge staff members gave differing accounts of the incident. Another child who uses a wheelchair got out of the home and allegedly crashed into a parked van, but no incident report was filed. In June, a child was administered the wrong medicine, and another child sustained a broken leg and bruising, although the causes remain unknown.
DCYF had received 11 complaints about the home and had found 24 licensing violations, leading the agency to suspend Weeping Ridge’s license.
In July, Rodriguez told the Spokesman that he requested an administrative hearing. DCYF confirmed that the Weeping Ridge license suspension is still in the appeals process. Rodriguez did not want to comment further for this story when reached via email.
Parents of children living at Weeping Ridge received a letter less than a week before the home was scheduled to close, leaving some families in limbo.
With Weeping Ridge closed, there are only 11 group homes statewide, with a total capacity for 83 medically intensive children. The majority of those homes are on the West Side, however, and there are just 19 spots in homes east of the Cascades.
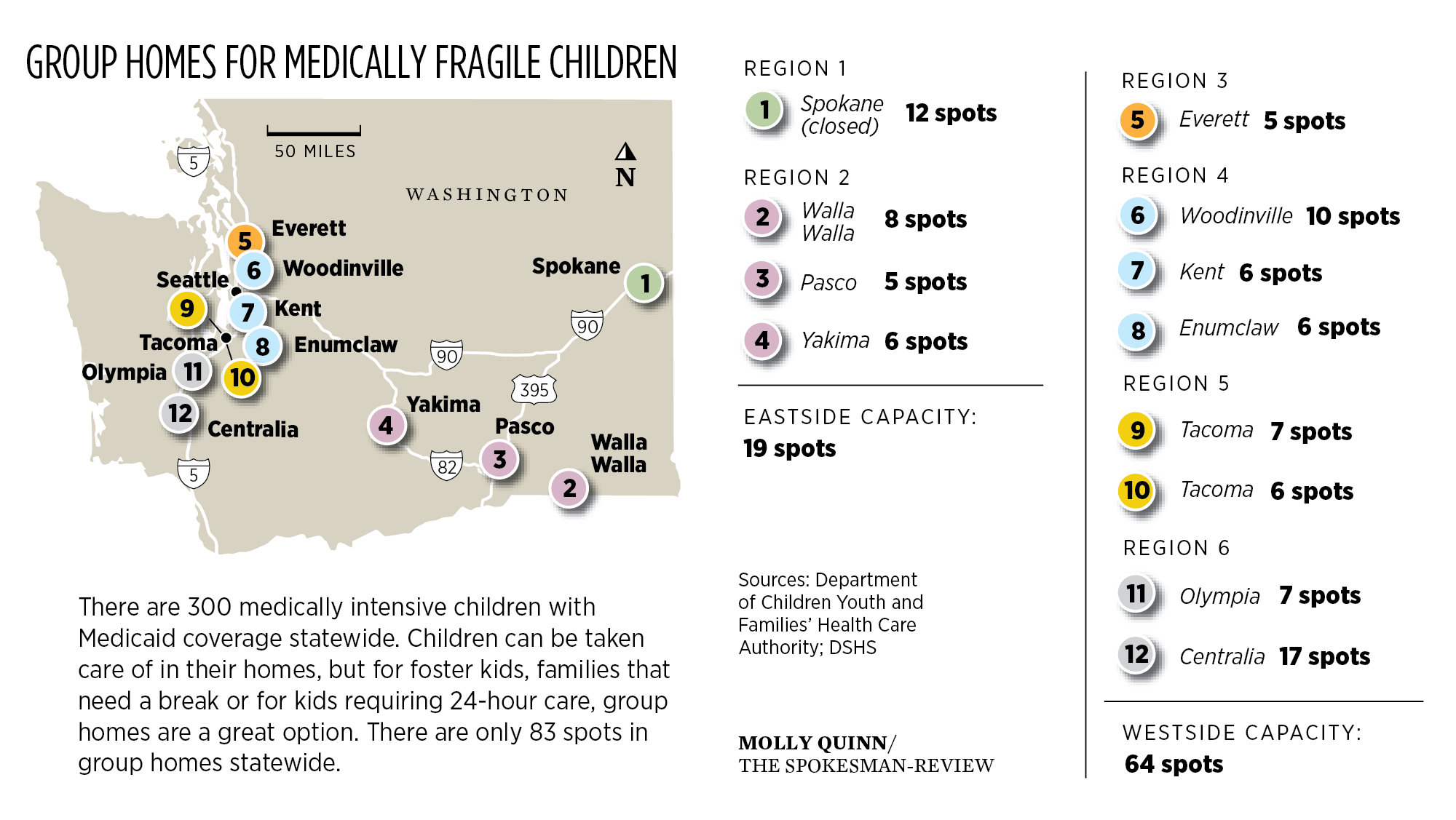
Not all group homes will take children with tracheostomies or more complex medical needs, so the numbers don’t exactly pair with each medically fragile child in the state. However, there are 300 children in the state considered medically intensive enrolled in a Medicaid fee-for-service or managed care plan.
When Weeping Ridge closed, the Groveses considered placing him with a medical foster parent or bringing him home. Sending him to a group home in Seattle was out of the question for them. Ultimately, they brought Isaac home, and the family is basically back where they were almost three years ago, except that they had only four days to hire nurses to fill their schedule.
For medically intensive children in the Spokane area, the nearest group home now is in Pasco, 135 miles away. If kids cannot be placed with their families or at group homes, they often go to the pediatric intensive care unit. Keeping kids out of hospitals for long-term care is a priority for every state agency that administers benefits for these kids.
“It’s not appropriate for these children to be in hospitals when they don’t need to be there, and to … ‘grow up in the hospital setting.’ That’s not what we’re here to support,” said Gail Kreiger, clinical nurse specialist with the Health Care Authority. “We want to place these children in a private home or residence or in a group home, so that they get the care that they need.”
Fighting for their kids
Cierra spent half of her first year of life at Sacred Heart Medical Center as doctors continued to diagnose her with different ailments, disorders or weak organs. Eventually, she would have open heart surgery when she was 9 months old.
Sacred Heart has the only Level IV NICU in the region, meaning all medically intensive and complex infants are transferred there. The hospital started the Sunflower Program in 2007 to serve families with medically intensive children.
“We get referrals from physicians when there is a child with a serious or complex medical condition who will likely be in and out of the hospital quite frequently because of their conditions,” said Carolyn Ringo, a nurse on the program team.
Flaget connected with other families through the program. The Sunflower Program has nurses, a social worker, a child life specialist and a physician. Each family gets a care plan that details what a child likes, dislikes and needs for care.
“We do have a long-term relationship with the families for the most part, so when difficult decisions have to be made about goals for their child, we have a relationship, and we’re able to support them and help them with those decisions,” Ringo said.
Parents or guardians of medically fragile children get an overnight crash course in care before their child leaves the hospital. Flaget spent the night with Cierra in the hospital, and she showed the doctors she knew how to monitor Cierra’s oxygen levels and ensure her feeding tube stayed in place. After one practice run, Flaget and her daughter were sent home with medical equipment, and the family living room transformed into a hospital overnight.
Cierra’s parents had private insurance through her father Jamie’s work for the railroad. Flaget recalls being told that it would be easier for Cierra to receive the full amount of care she needed if neither she nor her husband worked at all, or if they made a little less money, which made little fiscal sense to her.
Flaget wanted to get Cierra enrolled for a Medicaid waiver that would give the family access to additional state funds for respite care or medical supplies. She was turned down numerous times before ultimately receiving the waiver she needed.

“I was basically Cierra’s administrator and advocate more so than her mom in so many ways,” she said. “I just think that I have this type A personality and … an amazing support system and an amazing partner, and it still almost broke me so many times. But I’m just thinking, even as well as we were doing, eventually I don’t know if I could have kept doing it. So I feel really passionate that there are also solutions. I think those group homes are really important, because even really high-functioning families – it’s really taxing.”
Dakota, the Flagets’ oldest daughter, recalls all of her baby sister’s machines beeping in their living room. She would wake up early to see who the night nurses were, she recalls. Dakota, who was a toddler at the time, still remembers the fire trucks crowding their driveway when they had to call 911 when Cierra needed emergency transport to the hospital.
The Flagets live north of Spokane, in the woods off a gravel road. Their remote location did not help Flaget in her search for nurses, and it was not until Cierra was 2 years old that she finally established a nursing routine.

Even using all of her nursing hours, Flaget was the sole caregiver for Cierra all day Sunday until 10 p.m., which meant she rarely left the living room. Jamie Flaget traveled a lot for his railroad job, but the couple also worked to ensure that Dakota was able to have a childhood outside their home, which meant splitting duties, one taking Dakota out and the other staying in with Cierra when necessary.
‘Your new norm’
Maren Gibson, Owen’s mother, sounds like a medical professional when she talks about her son. She not only cares for him, but is his fiercest advocate. She has countless stories of being the “expert” in the room on her son’s care, despite her lack of medical education.
Gibson is a special education teacher in the Cheney School District, but nothing in her educational background prepared her to care for Owen, who was born at .Holy Family Hospital. Gibson recalls the panic and rush of a MedStar ambulance, with a specialized team, taking Owen to the NICU at Sacred Heart. Medical staff didn’t think he would survive, but he stayed at the NICU for 47 days.

Gibson, who is dedicated to her teaching career, was told by multiple people at the hospital that she could stop working altogether, which she refused.
“I’m not going to make the state pay for me, my son and my daughter,” she said. “I said, ‘I work, and I have that insurance, and that’s what I’ve always done.’ That’s the primary, and the state is secondary. I remember that so clearly.”
She did use family medical leave to stay home with Owen in his first year.
Eventually, Owen’s care became a family effort. His big sister, Emma, learned how to suction Owen’s breathing tube and care for her brother alongside her mother, her father and her younger sister, Ella.
The family’s dynamics shifted with Owen at home. There’s always a parent at home if there are no nurses. Nurses are constantly coming in and out of the house, and Gibson remembers what staff at the hospital told her as they prepared to bring Owen home: this would be their “new normal.”

“When people ask me ‘What are you going to do this weekend?’ I want to go, ‘Are you kidding me?’ ” she said. “Because I have to say pretty much stay home, and if not, then it means I have to leave my husband at home, or he goes and takes my daughters to some weddings and I stay home. That’s what families have to do.”
Owen is double-covered with health insurance from Gibson’s job and the Medicaid waiver. The Gibsons hired one of their nurses to cover a 10-hour respite shift two weekends each month, so the family can go out without having to take Owen and all of his equipment. Even still, Owen receives 16 hours of nursing every day, meaning the Gibsons are covering the 5 to 10 p.m. shift in the evening during the week, as well as 7 a.m. to 10 p.m. on the weekends, except when there is a respite day.

Technically, when families move home from the hospital, it is possible for them to receive up to 24 hours of nursing, easing them into caring for their child too.
“The state plan says up to 16 hours a day. We look at exceptions. If it’s 24 hours a day, they generally need to go to a group care facility, so we can ensure the coverage is there,” said Doris Barrett with the Developmental Disabilities Administration.
Of the 105 children on the state’s fee-for-service Medicaid plan, 66 have the waiver. Twenty-four of those children live in the Spokane region, meaning those children could temporarily stay in a group care home if their family needs a break or to travel.
In addition to caring for their children’s medical needs, parents become experts in scheduling medical appointments and home care and planning for deliveries of medical equipment. Beyond the day-to-day planning, families must go through reviews and reapplication processes on a six-month and an annual basis, depending on the benefits.
Both Owen and Isaac qualify for services from DDA, the agency that determines how many hours of nursing a family qualifies for. These reviews are now administered every six months by DDA. Gibson said these meetings can be stressful, especially due to the possibility that care hours could be cut. Medicaid benefits also must be renewed annually, with updated paperwork.
“The family needs to be aware that if they receive notification about documents, paperwork is being requested to maintain their eligibility, that they respond timely to those request,” said the Health Care Authority’s Kreiger.
Some medically fragile children do improve, especially if they are born with isolated conditions that can be treated with surgeries or procedures over time. Others like Owen and Isaac require 24-hour care and have not yet become mobile. Between the financial and emotional stress of caring for medically intensive children, family structures can also crumble.

“I heard from other parents how tough it is and how hard it is, and I get it, I know,” Gibson said. “I didn’t choose for the medical equipment to get so advanced that it would save my child’s life either, I didn’t choose that. Would I have been sad had he passed? Absolutely, but I live a day-to-day grief that nobody understands because it’s like a roller coaster: the ups and downs, the ins and outs, and the demands and the questions and the financial burden.”
Pushing ahead
Sam Grove could be a journalist.
When Weeping Ridge closed, he requested a list of appropriate group homes in the state and started dialing numbers.
Down the list of group homes in the state, Ashley House becomes a recurring name. The nonprofit runs five care homes for medically fragile kids on the West Side.
This summer, Grove reached out to Mike Pugsley, director of development at Ashley House. He helped coordinate meetings with Ashley House and Sunflower Program staff members to get the ball rolling. Grove has also met with several lawmakers and searched for potential properties that could become a group home.
Group care homes are often embedded into a neighborhood, in a house that has been renovated with wider hallways, wheelchair ramps for accessibility and medical equipment compatibility.
Ashley House is working to develop a finance plan and find local partners in order to purchase the property and open a home, Pugsley said.
They need nearly $1 million to buy and renovate the site. Grove started a GoFundMe page for the Ashley House Spokane project, and he has asked lawmakers to consider funding the project as well.
Group homes typically operate on Medicaid and private health insurance reimbursement from their clients, but that does not mean funding is not a challenge.
“I’m chomping at the bit to get (a) property so we can get going,” Pugsley said.
It would likely take eight to nine months to get the property renovated and ready to house kids, Pugsley said, and he said they would like to license a facility in Spokane for eight patients.
Pugsley understands well the intersection of policy and care for medically fragile kids, after years advocating for increased funding for home care in the statehouse. There’s a fine line between in-home care and group-home care for medically intensive children. Sometimes children at the group care homes are only there a few years, and then are reintegrated into their family homes.
While parents generally would prefer not to institutionalize their children, group homes can fill a gap in services when necessary.
“Our primary wish and function is we want kids to live with their families,” Pugsley said. “So kids coming in, we start planning that with their families and thinking of it when we first meet them.”
Ashley House has worked with 800 families over 30 years, and Pugsley estimates that more than 50 percent of the kids Ashley House serves are eventually reunited or going to homes.
Grove hopes that the Legislature will consider granting Ashley House funds to help purchase property, too. He spoke with Spokane Rep. Marcus Riccelli, who is on both the Health Care and Wellness and Capital Budget committees, about state funding for a Spokane group home.
Riccelli said funds for a project could come through the Building Communities Fund or through member-requested projects. Next year is a supplemental budget year, however, meaning there is less money to go around.
“I think from a values perspective and from a monetary perspective, for the state to be a good steward, it seems like we should have one of these facilities so kids aren’t in the hospital when they don’t need to be,” he said.
Riccelli is open to seeing if they can help fund a group home in upcoming budget cycles, and said the community needs to have a conversation about the need for more housing options for medically fragile children and adults with disabilities.
“I am 100% on board with the conversation and looking for solutions for medically fragile kids and Spokane families here,” he said. “And I’m interested in a broader community conversation in housing for our vulnerable populations in general.”
A premonition
Cierra Flaget did not live to her sixth birthday.
Cami remembers taking her to the hospital for what would be the last time in August 2013. She just knew something was wrong. Cierra struggled to breathe, but emergency department physicians could not figure out what was wrong. Cami asked them to keep her overnight anyway.
She met her husband for a rare meal together before he left on a train, and driving back to the hospital to be with Cierra, she got a call.
“Is this Cierra’s mom?”
“What’s wrong?” Flaget responded.
Later, she recalls a premonition; she just knew, before the hospital had even called, that they had lost her.
This August, Cami and Dakota, now 14, sat in their living room, restored to its original state with a long couch, bright windows with forest views and comfortable chairs. It is hard to imagine the machines and noise of Cierra’s world that used to fill the room six years earlier.
Two years ago, the Flagets adopted Sun, a 15-year-old from China, who is deaf. The whole family is learning sign language. Flaget had always wanted to adopt, but after Cierra died, it took time before the family felt ready.
“When I got pregnant with Cierra, Dakota was so excited to have a sister … but she never got her playmate,” Flaget said. “It’s so beautiful for Jamie and I to watch Dakota and Sun outside, playing volleyball for hours at a time. She’s an incredible sister, and Cierra taught her so many things at a young age that we almost can’t articulate.
“I’m so grateful that she gets to be that again, and I’m so grateful that I get to parent another child again.”
arielled@spokesman.com