Northwest Passages event on ‘How to Make a Killing’ to explore the controversy behind the for-profit dialysis industry
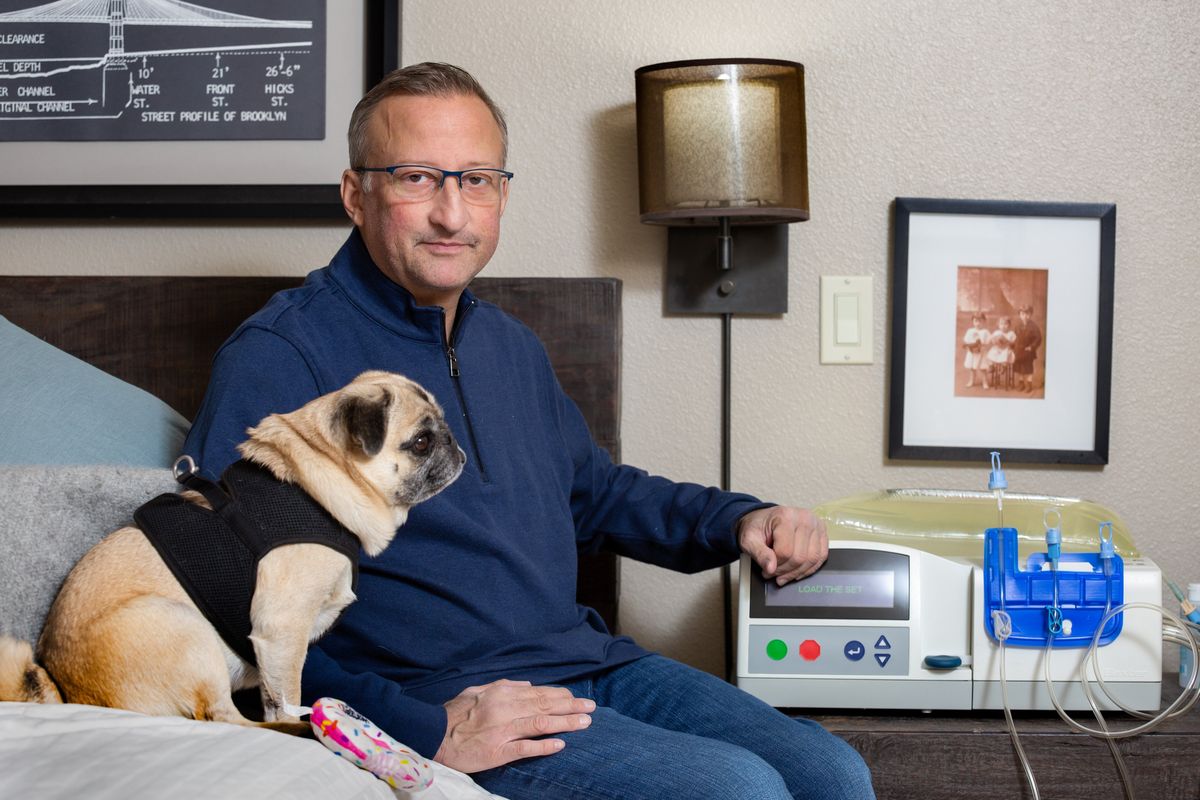
After being diagnosed with Lupus at 15, Andrew Storfer has had “40 years to prepare” for dialysis. But it was still a shock when he began the process of manually removing the toxins from his body earlier this year at age 53.
“You’re never fully prepared for it, and it was still super traumatic. It’s something I’ve been dreading my whole life,” he said.
Storfer will need to continue his nightly dialysis treatment for the rest of his life, or he could get a kidney transplant. A transplant from a deceased donor of his blood type could be more than three years away. Though long private about his medical condition, the Washington State University professor has started actively looking for a living donor.
Right now he feels “tethered” to his dialysis machine.
“I’m just treading water in my life. I want to move forward,” he said.
Storfer’s story is not unique. Over 37 million Americans have some type of renal disease. Of those, over 800,000 are currently diagnosed with renal failure. There are dialysis treatment centers in most cities and many small towns – taking up space in strip malls and business parks alike.
Dialysis has a unique place in American medicine as the only notable example of a treatment where insurance to pay for it is covered by the federal government. Even though programs like Medicare and Medicaid are required to cover dialysis treatments, the industry is still run on a for-profit basis.
Over 80% of dialysis centers are owned by two large for-profit companies: DaVita and Fresenius. As of last year, the federal government expends nearly $38 billion annually for dialysis patients – much of which is funneled into these two companies at a tidy profit for their shareholders.
The impact of the treatment’s commercialization is charted in the new book “How to Make a Killing,” by Tom Mueller. Like with many aspects of American health care, its for-profit nature can create perverse incentives that may keep patients away from care they need to live.
The United States has the lowest survival rate for dialysis patients of any industrialized nation. Twenty-two percent of dialysis patients die each year, according to Mueller’s research.
“That we allow some of our most defenseless citizens to be herded together and bled for profit, that we watch mutely as money taints medical ethics, that we accept and even celebrate greed when it’s airbrushed with the discredited ideologies of long-dead economies … dialysis in America is symptomatic of a chronic, society-wide condition,” Mueller writes in the book.
In association with The Spokesman-Review’s Northwest Passages book series, Mueller and Storfer will join a group of expert panelists to discuss the state of dialysis in the United States and the impact of “How to Make a Killing” on that industry.
Taking place at Gonzaga University’s Myrtle Woldson Center on Oct. 23, tickets for the event can be purchased at spokesman.com/northwest-passages/events.
What is dialysis?
In the book, Mueller describes the kidneys as the “architects of hemostasis” in the body.
Human bodies produce waste and byproduct that must be removed or they will build up and cause death. The kidneys are the primary organs taking this function – siphoning off these wastes toxic to the body and filtering them out through urine.
Before the advent of dialysis, an individual experiencing renal failure could not survive long.
Dialysis treatment was first developed during WWII and eventually evolved to its modern form – blood is pumped outside of the body into an artificial kidney where it is cleaned and returned to the body.
The process was lengthy, cumbersome and expensive, but it transformed a death sentence into a treatable disease. At the same time, dialysis is its own kind of hardship. It forces patients to be tied to a machine for large chunks of their life and to face all sorts of side effects.
As the American dialysis industry took shape in the United States, it developed into two sects. One based in Seattle promoted a nonprofit system of dialysis with longer, slow treatments done at home. Another based in Boston argued in-clinic, for-profit dialysis would be safer, make the treatment more available and be cheaper.
By the time the federal government agreed to insure all dialysis patients by 1972, the Boston sect had won out. Though paid for by the government, dialysis today remains a largely for-profit enterprise in America.
What for-profit dialysis does to its patients
Peter Laird was working as a doctor in 1998 when he was diagnosed with a kidney disease he initially believed to be benign. But by 2007, his kidney function had drastically fallen and he began dialysis.
As a doctor, he had admitted many patients who needed dialysis and knew how difficult it could be.
“I remember telling my wife, I see these people on dialysis just crash and burn all the time,” he said.
Now retired in Coeur d’Alene, Laird has spent much of his time conducting his own dialysis treatments at home. He’s back as an in-center patient, but Laird has done his dialysis at home for 11 years and at a center for six years off and on.
In his time at many clinics over the course of his 17-year journey with dialysis, Laird has seen many patients completely dependent on dialysis to survive who suffer because of the relatively speedy in-clinic treatments.
“In dialysis, they pull the fluid from the blood. And if you pull it off too rapidly, the patient’s blood pressure bottom’s out, they’ll get nauseous, they’ll get lightheaded, they’ll pass out, they’ll get cramps. I’ve seen people like that next to me. It’s a very perverse situation. It’s essentially introducing shock, which can damage all the organs in the body,” he said.
Laird blames the for-profit nature of the dialysis industry for these kind of preventable distresses during treatment.
“When the for-profit industry took over, they went for the biggest, baddest return on their money, as far as profit-wise. And that means shorter and shorter and shorter treatments.”
Laird believes nephrologists should be paid by hours of treatment, rather than the number of treatments they conduct.
“There’s a certain limit on how much fluid you can take off per hour. And if you exceed that, the mortality goes up substantially. The standard of care in American dialysis centers is based not on physiologic reasoning, but how many patients they can get in and out the door.”
A 2011 Fresenius memo uncovered by Mueller recommends their clinicians provide a “minimum dialysis treatment time of four hours.” That time in clinic can often be less for many patients.
In their response to the book, the other large dialysis corporation argued their “first consideration” is always “patient safety.”
“We are committed to providing a comfortable, therapeutic treatment environment for all patients,” reads the DaVita statement.
As a doctor, Laird has been afforded much more control over his own treatment than the average patient – at home and in the clinic. His treatments are longer, and he sets the parameters of the treatments based on his own recommendations, which are approved by a nephrologist.
Despite this control, Laird has had his own difficulties with the large dialysis conglomerates, which were highlighted in “How to Make a Killing.” The doctor declined to discuss these issues again for fear of “poking the tiger in the eye.”
In his book, Mueller states Laird was practicing dialysis at home but was provided equipment and supplies from a clinic. In at-home treatments, Laird began to suffer nausea and headaches, which he believed were caused by new equipment provided to him by the clinic.
Rather than providing new equipment, the clinic asked him to begin in-center treatment. Upon asking to be transferred to a new clinic, Laird was involuntarily discharged. He was later able to resume treatment at another clinic.
“If the dialysis companies can deal with a medical doctor like this, what must they do to the average patient?” Laird is quoted as asking in the book.
Laird’s story is one of many highlighted in “How to Make a Killing” where patients allege they were involuntarily discharged by their clinic when they did not need to be. Signaling the patient may be a danger to staff, an involuntary discharge at one clinic often makes it difficult to obtain treatment at another.
One nephrologist quoted in the story describes some staff members in the clinics as “prison camp guards.” Another said technicians are often “on a power trip.” At the same time, these employees are overworked, caring for many patients at a time, and can be underqualified – often only needing to graduate high school and receive some certification.
“Once they want to terminate a patient, they are skilled at having multiple employees document a one-sided story” nephrologist Dr. Jesse Goldman said in the book. “The story is always exaggerated. Not only is the documentation used as ‘evidence’ for the ejection but it also makes more difficult to place patients in the future since the extreme narrative scares away future units from taking a chance.”
A common theme among stories in the book is patients being specifically accused of threatening staff with a firearm as a pretext for an involuntary discharge. These accusations are denied by those interviewed in “How to Make a Killing.” A survey cited in the book found that between 2013 and 2020, there were 20 instances of gun-related aggression and five violence-related deaths at dialysis clinics in the United States.
If a patient is unable to find a clinic that will take them, they are forced to receive their dialysis treatments at an emergency room. Because of the frequency of their treatments, emergency departments only treat dialysis patients if their life is imminently in danger without it.
According to Mueller, a majority of those who are involuntarily discharged use Medicare or Medicaid, which provide much less profit than those covered by private insurance. In their written response to Mueller, DaVita disagreed.
“We welcome feedback to continually deliver the best care experience possible and strive to be a place of belonging for everyone in our center,” reads the company statement.
Mueller also notes a disproportionate number of those involuntarily discharged from dialysis centers are people of color, who are more likely to use government-funded treatment and are disproportionally in need of dialysis.
Storfer stressed that in his short time on dialysis, he has had a very positive experience from his clinic and medical providers.
“All the people I’ve encountered in terms of dialysis – nurses, nephrologists and technicians – all seem compassionate and caring,” he said.
But Storfer still has fears about the corporatization of the industry making his treatment more formulaic and less individualized.
“The providers at the clinic-level are all great, but the middle- and upper- management sees me not as a patient getting life-sustaining treatment, but as a number,” he said.
Storfer began his treatments in-clinic in August but moved to home treatment a month later. He relies on the clinic’s equipment and supply for peritoneal dialysis, which is generally seen as less invasive than the hemodialysis done in clinics.
The WSU professor hopes and plans that his need for dialysis treatment is a temporary one. He hopes to find a living kidney donor and is registered for transplant at Providence Sacred Heart Medical Center. Potential donors can learn more at his website, storferneedsakidney.org.
Whatever the future may hold, Storfer hopes to use his experience as a dialysis patient and a biology professor to be a science communicator to the public.
“I know how to talk to patients. Not only am I a professional teacher, but I am a patient and I’m also a scientist. I can talk on the same level as all the doctors, but I can also talk to the patients. I’m in a unique position where I can truly empathize because I’m going through what they’re going through,” he said. “I hope I can be an advocate and educator for people who may be falling prey to the corporate system.”